

There has been a lot of speculation, lately, about vaccines possibly being harmful and, in particular, causing autism. You know I work on HIV vaccine design, so there's no need to say where I stand on the need of vaccinations. No link has been found between the incidence of autism and vaccination. Of course, medicine is not an exact science. Outliers will always exist. The U.S. seem to be a special case, as the vaccination schedule in this country requires a high number of vaccine doses, yet the infant mortality rate is one of the highest among North America and European countries. However, take a close look at this graph:
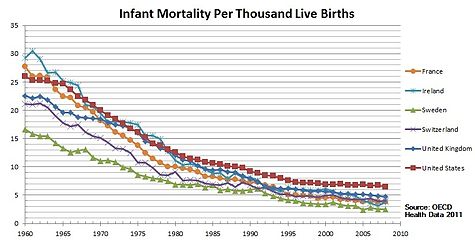
The countries with low mortality rate shown in this graph have a strict vaccination schedule, just like the U.S. On the other hand, what distinguishes them from the US is affordable health care. Countries with a high infant mortality rate are countries where poor people do not have access to vaccines and good health care. For the 3-million AIDS orphans living in sub-Saharan Africa a vaccine against HIV is the only hope they have to live into adulthood. It is quite easy for those of us who have a healthy life style and have access to food, medicines, and doctors on a daily basis, to say "no, thank you" to vaccines. But please, when you make your own decision about vaccines, do remember the millions of people for whom this is not a choice. And also remember: some children who are immunodefecient really cannot be vaccinated. They cannot contract any kind of disease, either, because their immune system is not working. However, if the majority of the people continue to get vaccinated, people who really cannot be vaccinated are still protected:
 |
| found on Facebook |
Back to autism. As you saw from my last post, ASD, or autism spectrum disorders, is indeed a puzzling disease and pinning down its etiology has been challenging. The genetics involve numerous genes and diverse pathways, implying that different mechanisms could potentially lead to ASD, particularly during fetal development. One thing that I recently discovered is a number of correlations found between infections in the mother during gestation and autism:
"Recent studies have highlighted a connection between infection during pregnancy and the increased risk of autism in the offspring. Parallel studies of cerebral spinal fluid, blood and postmortem brains reveal an ongoing, hyper-responsive inflammatory-like state in many young as well as adult autism subjects. There are also indications of gastrointestinal problems in at least a subset of autistic children [1]."In his review [1], Patterson makes a good summary of the relevant studies: for example, a permanent, inflammatory-like state has been found in postmortem examination of ASD affected brains. This was found at all ages, indicating that the state was established early in the development and maintained throughout the life-span of the ASD affected individual. These abnormalities expand to the central nervous system and the peripheral immune system affecting also the gastrointestinal tract:
"These findings include immune cell infiltrates present in the colon, ileum and duodenum, as well as increased T cell activation in the intestinal mucosa. These inflammatory changes are associated with autoimmune responses that could contribute to the observations of decreased mucosal integrity, or 'leaky gut' [1]."
"Abnormal activation of the immune system may also be involved in the etiology of autism. [. . .] Family members of autistic children, particularly the mothers, show a higher incidence of allergy or autoimmune diseases. Consistent with immune involvement are findings that maternal infection is a risk factor for autism [2]."In conclusion, there is a correlation between immune abnormalities and ASD, and the immune abnormalities propagate to the brain and the gastrointestinal tract. However, it is unclear if these abnormalities cause the behavioral symptoms of ASD or if they are a secondary effect. The health and well-being of our immune system has such deep, profound effects on the central nervous system. The two interact very closely together: stress and the general emotional status, for example, can affect immunity; vice versa, the immune system can influence behavior. Both our brain and our immune system constantly learn and readapt to the surrounding environment (for example, our immune system learns to recognize new pathogens throughout our lifetime), which makes them prone to life-long epigenetic changes induced by environmental factors such as stress and disease. It's not a coincidence that:
"Immune dysregulation has also been implicated in the etiology of a variety of neurodegenerative, psychiatric, and neurodevelopmental disorders, including Parkinson, Huntington, and Alzheimer diseases, multiple sclerosis, major depression, schizophrenia, and addiction [2]."Hsiao et al. [2] addressed the open question of whether the immunological abnormalities cause ASD-like behaviors in a mouse model. They induced ASD in mouse offspring through "maternal immune activation" (MIA): the immune system of pregnant mice was altered and then the offsprings of the altered mice that were behaviorally abnormal was compared to the offsprings of the controls. The behaviorally abnormal MIA offsprings exhibited core behavioral symptoms of autism, including increased repetitive behaviors, decreased social interactions, and increased anxiety. Hsiao et al. found several abnormalities in the immune system of these MIA offsprings: levels of regulatory T-cells were decreased and CD4+ T-cells were hyper-responsive. These abnormalities could not be transferred to healthy mice through a bone marrow from the MIA mice. However, when irradiated and transplanted with immunologically normal bone marrow, many of the behavioral abnormalities stopped. This would suggest that the immunological dysregulation causes the ASD-like behaviors.
"It is striking that in a mouse model of an autism environmental risk factor that exhibits the cardinal behavioral and neuropathological symptoms of autism, there is also permanent peripheral immune dysregulation. This finding provides the opportunity to explore molecular mechanisms underlying the relationship between brain dysfunction and altered immunity in the manifestation of abnormal behavior. Furthermore, this finding provides a platform for investigating how prenatal challenges can program long-term postnatal immunity, health, and disease. Maternal insult-mediated epigenetic modification in HSC and progenitor cells is one possible mechanism for how effects may be established by transient environmental changes yet persist permanently into adulthood. However, the BM transplant results suggest that the peripheral environment of the MIA offspring is also critical for maintaining a permanently modified immune state [2]."We will never be able to prove or disprove a direct causal relation between vaccines and autism: if a child develops ASD after vaccination, unfortunately, we cannot rewind time and see if the same child, without the vaccine, would've never developed ASD in his/her lifetime. ASD typically develops in infancy, which is when the bulk of vaccines are administered. The risk of ASD is much higher (see last week's post) if there's already a family member with ASD, siblings in particular. And given the deep, complex interactions and reciprocal influence between the nervous system and the immune system it is quite possible that a sudden change in the immune system could cause some level of disruption in the nervous system. However, if the immune system is primed to such risk, a virus or any other pathogen, which cause changes in the immune system just like a vaccine does, could also cause similar disruptions. On the other hand, vaccines can potentially prevent infections that, according to these studies, do increase the risk of ASD in the baby during the first trimester of gestation.
So, as always: Read the literature, talk to your doctor, possibly to more than one, consider your family's medical history, and, whatever decision you make, make sure it is an informed decision.
[1] Patterson, PH (2011). Maternal infection and immune involvement in autism Trends in Molecular Medicine DOI: 10.1016/j.molmed.2011.03.001
[2] Hsiao EY, McBride SW, Chow J, Mazmanian SK, & Patterson PH (2012). Modeling an autism risk factor in mice leads to permanent immune dysregulation. Proceedings of the National Academy of Sciences of the United States of America, 109 (31), 12776-81 PMID: 22802640

